Confirmation
CONFIRM Endotracheal Tube (ETT) placement by:
- Visualization of end tidal waveform on monitor (may be a delay of 2-3 breaths)
- Visualization of adequate chest rise with manual breath
- Presence of condensation in the ETT on exhalation
- Confirmation of breath sounds on auscultation
- Obtain chest x- ray
- Obtain blood gas (capillary/venous blood gas if arterial sample not accessible)
Airway Securement
For securing an Endotracheal Tube (ETT), two people are required in the process: one person should hold the tube in place, while the other person secures it.
For ETT with a size less than 5.0, a Neobar is recommended.
- When sizing the Neobar, ensure a proper fit by first measuring from the midline of the nose to the opening of the ear canal by using the Neobar tape. Once the correct size is identified, position the Neobar between the ears, running it from one ear to the other. Place the bar between the lips, ensuring it is centered. Avoid pulling or stretching the Neobar too tight. To secure the Neobar and ETT, use one long piece of tape and wrap once around the Neobar before you begin to secure the ETT. As you wrap the tape around the ETT, ensure each wrap overlaps the previous one for added security, mimicking a candy cane design. Pay special attention to securing the tip of the Neobar, as this is where the tape tends to stretch - consider wrapping more than once if needed. Finish by making a small courtesy tab at the end to allow for easy removal in case any repositioning of the ETT is necessary.

For ETT sizes greater than and equal to 5.0, it is recommended to use an Anchorfast.
If a Neobar or Anchorfast cannot be used due to facial trauma, burns, or similar injuries, it is recommended to use twill ties.
Neotech. Airway Securement. Available from: https://www.neotechproducts.com/product/neobar/.
Airway Securement [Internet]. 2019. Available from: https://www.youtube.com/watch?v=0blEXPZZQ2Y.
Ventilation Goals
Goals of ventilation should be :
- Normocarbia (ETCO2/ PaCO2: 35 to 45 mmHg)
- Saturations >92%
References:
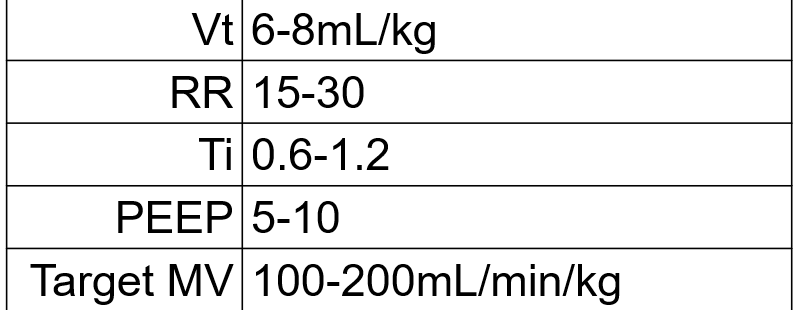
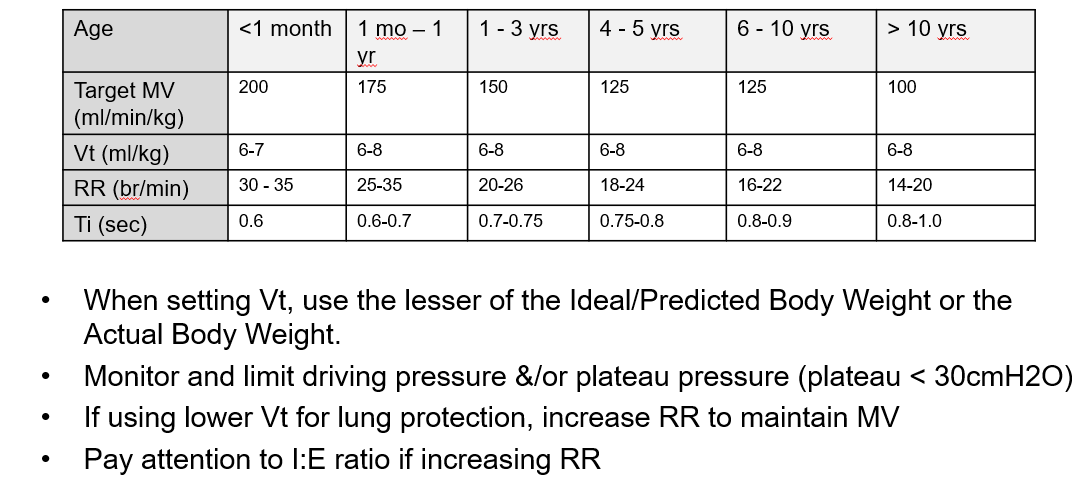
Vt: Tidal Volume
RR: Respiratory Rate
Ti: Insipiratory Time
PEEP: Positive End-expiratory Pressure
MV: Minute Ventilation
IBW: Ideal Body Weight
I:E: Inspiratory : Expiratory
BC Children’s Hospital PICU Physicians RT. Acute Ventilation in Pediatrics [Internet]. 2024. Available from:
Maintenance
Ongoing sedation and analgesia:
- Morphine 10 to 20 mcg/kg/hour IV
- Midazolam 100 to 200 mcg/kg/hour IV
- Dexmedetomidine 0.1-1mcg/kg/hr IV (can be added if available)
Consider ongoing paralytic medications :
- Rocuronium – intermittent IV boluses of 1mg/kg as required while ensuring adequate sedation